- Home
- Tezapride M2
Tezapride M2

Tezapride M2
TM TEZAPRIDE M2 Metformin Hydrochloride Prolonged- release and Glimepiride Tablets IP (500mg+2mg)
COMPOSITION
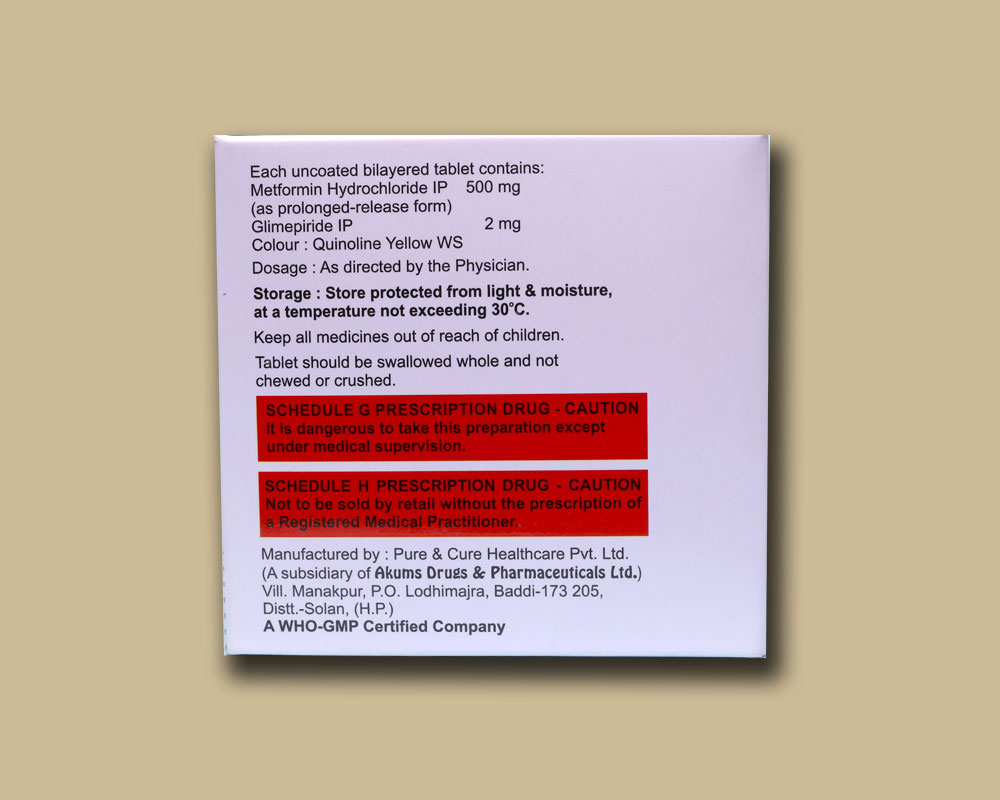
Each uncoated bilayered tablet contains:
Metformin Hydrochloride IP 500 mg
(as prolonged-release form)
Glimepiride IP
2 mg
Colour: Quinoline Yellow WS
PHARMACEUTICAL FORM
Uncoated bilayered tablet
THERAPEUTIC INDICATION
For patients with type 2 diabetes mellitus when diet, exercise & the single agent do not result in adequate glycemic control.
DOSAGE AND ADMINISTRATION
Posology
Adults:
The recommended dose is 1 tablet once daily or as directed by the Physician.
Special population:
Children & adolescents below the age of 18 years: The safety and effectiveness in pediatric patients have not been established. Hence, it is contraindicated in children & adolescents below the age of 18 years.
Elderly: Start with lowest dose in elderly patients due to higher risks of lactic acidosis, poor renal and hepatic functions.
In patients with renal impairment: Glimepiride/Metformin tablet is not recommended in patients with renal impairment and renal failure.
In patients with hepatic impairment: Glimepiride/Metformin tablet is not recommended in patients with hepatic impairment and hepatic failure.
Method of administration: For oral administration only. Glimepiride/Metformin tablets must be swallowed whole and never split, crushed or chewed.
CONTRAINDICATIONS
It is contraindicated in patients with known hypersensitivity to the any of the active substance(s), or to any other component of this product.
Glimepiride is contraindicated in patients with the following conditions:
In patients hypersensitive to glimepiride, other sulfonylureas, other sulfonamides.
In pregnant and breast-feeding women.
No experience has been gained concerning the use of glimepiride in patients with severe impairment of liver function and in dialysis patients. In patients with severe impairment of hepatic function, change-over to insulin is indicated, not least to achieve optimal metabolic control.
Metformin is contraindicated in patients with the following conditions:
Renal impairment (e.g., serum creatinine levels ≥1.5 mg/dL for men, ≥1.4 mg/dL for women or abnormal creatinine clearance), which may also result from conditions such as cardiovascular collapse (shock), acute myocardial infarction, and septicemia.
Acute or chronic metabolic acidosis, including diabetic ketoacidosis. Diabetic ketoacidosis should be treated with insulin.
SPECIAL WARNINGS AND PRECAUTIONS FOR USE
Warning: Lactic Acidosis
Lactic acidosis is a rare, but serious, complication that can occur due to metformin accumulation. The risk increases with conditions such as sepsis, dehydration, excess alcohol intake, hepatic impairment, renal impairment, and acute congestive heart failure. The onset of lactic acidosis is often subtle, accompanied only by nonspecific symptoms such as malaise, myalgia’s, respiratory distress, increasing somnolence, and nonspecific abdominal distress. Laboratory abnormalities include low pH, increased anion gap, and elevated blood lactate. If acidosis is suspected, Glimepiride/Metformin tablets should be discontinued and the patient hospitalized immediately.
This tablet should be administered carefully in patients who are receiving other antidiabetic drugs because hypoglycemia may occur.
Glimepiride
Hypoglycemia
All sulphonylurea drugs are capable of producing severe hypoglycemia. Proper patient selection, dosage, and instructions are important to avoid hypoglycemic episodes. When a patient stabilized on any diabetic regimen, is exposed to stress such as fever, trauma, infection, or surgery, a temporary loss of glycemic control may occur. At such times, it may be necessary to withhold the diabetic regime and temporarily administer insulin.
Hypersensitivity Reactions
There have been postmarketing reports of hypersensitivity reactions in patients treated with glimepiride, including serious reactions such as anaphylaxis, angioedema, and Stevens-Johnson syndrome. If a hypersensitivity reaction is suspected, promptly discontinue glimepiride, assess for other potential causes for the reaction, and institute alternative treatment for diabetes.
Hemolytic Anemia
Sulfonylureas can cause hemolytic anemia in patients with glucose 6-phosphate dehydrogenase (G6PD) deficiency. Because glimepiride is a sulfonylurea, use caution in patients with G6PD deficiency and consider the use of a non-sulfonylurea alternative. There are also postmarketing reports of hemolytic anemia in patients receiving glimepiride who did not have known G6PD deficiency.
Increased Risk of Cardiovascular Mortality with Sulfonylureas
The administration of oral hypoglycemic drugs has been reported to be associated with increased cardiovascular mortality as compared to treatment with diet alone or diet plus insulin. This warning is based on the study conducted by the University Group Diabetes Program (UGDP), a long-term, prospective clinical trial designed to evaluate the effectiveness of glucose-lowering drugs in preventing or delaying vascular complications in patients with non-insulin-dependent diabetes. The study involved 823 patients who were randomly assigned to one of four treatment groups.
UGDP reported that patients treated for 5 to 8 years with diet plus a fixed dose of tolbutamide (1.5 grams per day) had a rate of cardiovascular mortality approximately 2-1/2 times that of patients treated with diet alone. A significant increase in total mortality was not observed, but the use of tolbutamide was discontinued based on the increase in cardiovascular mortality, thus limiting the opportunity for the study to show an increase in overall mortality. Despite controversy regarding the interpretation of these results, the findings of the UGDP study provide an adequate basis for this warning. The patient should be informed of the potential risks and advantages of glimepiride and of alternative modes of therapy.
Although only one drug in the sulfonylurea class (tolbutamide) was included in this study, it is prudent from a safety standpoint to consider that this warning may also apply to other oral hypoglycemic drugs in this class, in view of their close similarities in mode of action and chemical structure.
Macrovascular Outcomes
There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with glimepiride or any other anti-diabetic drug.
Metformin
Lactic acidosis
Lactic acidosis is a serious, metabolic complication that can occur due to metformin accumulation during treatment with metformin and is fatal in approximately 50% of cases. Lactic acidosis may also occur in association with a number of pathophysiologic conditions, including diabetes mellitus, and whenever there is significant tissue hypoperfusion and hypoxemia. Lactic acidosis is characterized by elevated blood lactate concentrations (>5 mmol/L), decreased blood pH, electrolyte disturbances with an increased anion gap, and an increased lactate/pyruvate ratio. When metformin is implicated as the cause of lactic acidosis, metformin plasma levels >5 µg/mL are generally found. The reported incidence of lactic acidosis in patients receiving metformin hydrochloride is approximately 0.03 cases/1000 patient years, with approximately 0.015 fatal cases/1000 patient-years. In more than 20,000 patient-years exposure to metformin in clinical trials, there were no reports of lactic acidosis.
Reported cases have occurred primarily in diabetic patients with significant renal impairment, including both intrinsic renal disease and renal hypoperfusion, often in the setting of multiple concomitant medical/surgical problems and multiple concomitant medications. Patients with congestive heart failure requiring pharmacologic management, particularly when accompanied by hypoperfusion and hypoxemia due to unstable or acute failure, are at increased risk of lactic acidosis. The risk of lactic acidosis increases with the degree of renal dysfunction and the patient’s age. The risk of lactic acidosis may, therefore, be significantly decreased by regular monitoring of renal function in patients taking Metformin. In particular, treatment of the elderly should be accompanied by careful monitoring of renal function. Metformin treatment should not be initiated in any patient unless measurement of creatinine clearance demonstrates that renal function is not reduced. In addition, Metformin should be promptly withheld in the presence of any condition associated with hypoxemia, dehydration, or sepsis.
Because impaired hepatic function may significantly limit the ability to clear lactate, metformin should generally be avoided in patients with clinical or laboratory evidence of hepatic impairment. Patients should be cautioned against excessive alcohol intake when taking metformin, because alcohol potentiates the effects of metformin on lactate metabolism. In addition, metformin should be temporarily discontinued prior to any intravascular radio contrast study and for any surgical procedure necessitating restricted intake of food or fluids. Use of topiramate, a carbonic anhydrase inhibitor, in epilepsy and migraine prophylaxis may frequently cause dose-dependent metabolic acidosis (In controlled trials, 32% and 67% for adjunctive treatment in adults and pediatric patents, respectively, and 15 to 25% for monotherapy of epilepsy, with decrease in serum bicarbonate to less than 20 mEq/L; 3% and 11% for adjunctive treatment in adults and pediatric patents, respectively, and 1 to 7% for monotherapy of epilepsy, with decrease in serum bicarbonate to less than 17 mEq/L) and may exacerbate the risk of metformin-induced lactic acidosis. The onset of lactic acidosis often is subtle, and accompanied only by nonspecific symptoms such as malaise, myalgia’s, respiratory distress, increasing somnolence, and nonspecific abdominal distress. There may be associated hypothermia, hypotension, and resistant bradyarrhythmias with more marked acidosis.
Patients should be educated to promptly report these symptoms should they occur. If present, metformin should be withdrawn until lactic acidosis is ruled out. Serum electrolytes, ketones, blood glucose, blood pH, lactate levels, and blood metformin levels may be useful. Once a patient is stabilized on any dose level of metformin, gastrointestinal symptoms, which are common during initiation of therapy, are unlikely to recur. Later occurrence of gastrointestinal symptoms could be due to lactic acidosis or other serious disease. Levels of fasting venous plasma lactate above the upper limit of normal but less than 5 mmol/L in patients taking metformin do not necessarily indicate impending lactic acidosis and may be explainable by other mechanisms, such as poorly-controlled diabetes or obesity, vigorous physical activity, or technical problems in sample handling. Lactic acidosis should be suspected in any diabetic patient with metabolic acidosis lacking evidence of ketoacidosis (ketonuria and ketonemia). Lactic acidosis is a medical emergency that must be treated in a hospital setting. In a patient with lactic acidosis who is taking metformin, the drug should be discontinued immediately and general supportive measures promptly instituted. Because metformin hydrochloride is dialyzable (with a clearance of up to 170 mL/min under good hemodynamic conditions), prompt hemodialysis is recommended to correct the acidosis and remove the accumulated metformin. Such management often results in prompt reversal of symptoms and recovery.
Monitoring of Renal Function
Metformin is substantially excreted by the kidney, and the risk of metformin accumulation and lactic acidosis increases with the degree of renal impairment. Therefore metformin is contraindicated in patients with renal impairment.
Before initiation of metformin and at least annually thereafter, renal function should be assessed and verified as normal. In patients in whom development of renal dysfunction is anticipated (e.g., elderly), renal function should be assessed more frequently and metformin discontinued if evidence of renal impairment is present. Metformin treatment should not be initiated in patients ≥ 80 years of age unless measurement of
creatinine clearance demonstrates that renal function is not reduced, as these patients are more susceptible to developing lactic acidosis. Use of concomitant medications that may affect renal function or metformin disposition – Concomitant medication(s) that may affect renal function or result in significant hemodynamic change or may interfere with
the disposition of metformin, such as cationic drugs that are eliminated by renal tubular secretion, should be used with caution. Radiological studies and surgical procedures: Radiologic studies involving the use of intravascular iodinated contrast materials (for example, intravenous urogram, intravenous cholangiography, angiography, and computed tomography) can lead to acute alteration of renal function and have been associated with lactic acidosis in patients receiving metformin. Therefore, in patients in whom any such study is planned, metformin should be temporarily discontinued at the time of or prior to the procedure, and withheld for 48 hours subsequent to the procedure and reinstituted only after renal function has been re-evaluated and found to be
normal. Metformin therapy should be temporarily suspended for any surgical procedure (except minor procedures not associated with restricted intake of food and fluids) and should not be restarted until the patient’s oral intake has resumed and renal function has been evaluated as normal.
Cardiovascular collapse (shock) from whatever cause, acute congestive heart failure, acute myocardial infarction and other conditions characterized by hypoxemia have been associated with lactic acidosis and may
Hypoxic States
also cause prerenal azotemia. When such events occur in patients on metformin therapy, the drug should be promptly discontinued.
Alcohol Intake
Alcohol is known to potentiate the effect of metformin on lactate metabolism. Patients, therefore, should be warned against excessive alcohol intake while receiving metformin.
Impaired Hepatic Function
Because impaired hepatic function has been associated with some cases of lactic acidosis metformin should generally be avoided in patients with clinical or laboratory evidence of hepatic disease.
Vitamin B12 Levels
In controlled, 29-week clinical trials of immediate release metformin, a decrease to subnormal levels of previously normal serum Vitamin B12 levels, without clinical manifestations, was observed in approximately 7% of patients. Such decrease, possibly due to interference with B12 absorption from the B12-intrinsic factor complex, is, however, very rarely associated with anemia and appears to be rapidly reversible with discontinuation of metformin or Vitamin B12 supplementation. Measurement of hematologic parameters on an annual basis is advised in patients on metformin and any apparent abnormalities should be appropriately investigated and managed. Certain individuals (those with inadequate Vitamin B12 or calcium intake or absorption) appear to be predisposed to developing subnormal Vitamin B12 levels. In these patients, routine serum Vitamin B12 measurements at two-to three-year intervals may be useful.
Hypoglycemia
Hypoglycemia does not occur in patients receiving metformin alone under usual circumstances of use, but could occur when caloric intake is deficient, when strenuous exercise is not compensated by caloric supplementation, or during concomitant use with other glucose-lowering agents (such as sulfonylureas and insulin) or ethanol. Elderly, debilitated, or malnourished patients, and those with adrenal or pituitary insufficiency or alcohol intoxication are particularly susceptible to hypoglycemic effects. Hypoglycemia may be difficult to recognize in the elderly, and in people who are taking beta-adrenergic blocking drugs.
Macrovascular Outcomes
There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with metformin or any other oral anti-diabetic drug.
DRUG INTERACTION
Glimepiride
Drugs affecting Glucose Metabolism
A number of medications affect glucose metabolism and may require Glimepiride dose adjustment and particularly close monitoring for hypoglycemia or worsening glycemic control.
The following are examples of medications that may increase the glucose-lowering effect of sulfonylureas including Glimepiride, increasing the susceptibility to and/or intensity of hypoglycemia: oral anti-diabetic medications, pramlintide acetate, insulin, angiotensin converting enzyme (ACE) inhibitors, H2 receptor antagonists, fibrates, propoxyphene, pentoxifylline, somatostatin analogs, anabolic steroids and androgens, cyclophosphamide, phenyramidol, guanethidine, fluconazole, sulfinpyrazone, tetracyclines, clarithromycin, disopyramide, quinolones, and those drugs that are highly protein-bound, such as fluoxetine, nonsteroidal anti-inflammatory drugs, salicylates, sulfonamides, chloramphenicol, coumarins, probenecid and monoamine oxidase inhibitors. When these medications are administered to a patient receiving glimepiride, monitor the patient closely for hypoglycemia. When these medications are withdrawn from a patient receiving Glimepiride, monitor the patient closely for worsening glycemic control.
The following are examples of medications that may reduce the glucose-lowering effect of sulfonylureas including glimepiride, leading to worsening glycemic control: danazol, glucagon, somatropin, protease inhibitors, atypical antipsychotic medications (e.g., olanzapine and clozapine), barbiturates, diazoxide, laxatives, rifampin, thiazides and other diuretics, corticosteroids, phenothiazines, thyroid hormones, estrogens, oral contraceptives, phenytoin, nicotinic acid, sympathomimetics (e.g., epinephrine, albuterol, terbutaline), and isoniazid. When these medications are administered to a patient receiving glimepiride, monitor the patient closely for worsening glycemic control. When these medications are withdrawn from a patient receiving glimepiride, monitor the patient closely for hypoglycemia.
Beta-blockers, clonidine, and reserpine may lead to either potentiation or weakening of glimepiride’s glucose-lowering effect.
Both acute and chronic alcohol intake may potentiate or weaken the glucose-lowering action of glimepiride in an unpredictable fashion.
The signs of hypoglycemia may be reduced or absent in patients taking sympatholytic drugs such as beta-blockers, clonidine, guanethidine, and reserpine.
Miconazole
A potential interaction between oral miconazole and sulfonylureas leading to severe hypoglycemia has been reported. Whether this interaction also occurs with other dosage forms of miconazole is not known.
Cytochrome P450 2C9 Interactions
There may be an interaction between glimepiride and inhibitors (e.g., fluconazole) and inducers (e.g., rifampin) of cytochrome P450 2C9. Fluconazole may inhibit the metabolism of glimepiride, causing increased plasma concentrations of glimepiride which may lead to hypoglycemia. Rifampin may induce the metabolism of glimepiride, causing decreased plasma concentrations of glimepiride which may lead to worsening glycemic control.
Concomitant Administration of Colesevelam
Colesevelam can reduce the maximum plasma concentration and total exposure of glimepiride when the two are coadministered. However, absorption is not reduced when glimepiride is administered 4 hours prior to
colesevelam. Therefore, glimepiride should be administered at least 4 hours prior to colesevelam.
Metformin
Carbonic Anhydrase Inhibitors
Topiramate or other carbonic anhydrase inhibitors (e.g., zonisamide, acetazolamide or dichlorphenamide) frequently decrease serum bicarbonate and induce non-anion gap, hyperchloremic metabolic acidosis. Concomitant use of these drugs may induce metabolic acidosis. Use these drugs with caution in patients treated with metformin, as the risk of lactic acidosis may increase.
Cationic Drugs
Cationic drugs (e.g., amiloride, digoxin, morphine, procainamide, quinidine, quinine, ranitidine, triamterene, trimethoprim, or vancomycin) that are eliminated by renal tubular secretion theoretically have the potential for interaction with metformin by competing for common renal tubular transport systems. Although such interactions remain theoretical (except for cimetidine), careful patient monitoring and dose
adjustment of metformin and/or the interfering drug is recommended in patients who are taking cationic medications that are excreted via the proximal renal tubular secretory system.
Drugs Affecting Glycemic Control
Certain drugs tend to produce hyperglycemia and may lead to loss of glycemic control. These drugs include the thiazides and other diuretics, corticosteroids, phenothiazines, thyroid products, estrogens, oral contraceptives, phenytoin, nicotinic acid, sympathomimetics, calcium channel blockers, and isoniazid. When such drugs are administered to a patient receiving metformin, the patient should be closely observed for loss of blood glucose control. When such drugs are withdrawn from a patient receiving metformin, the patient should be observed closely for hypoglycemia.
Concomitant use of Metformin not recommended
Alcohol: Alcohol intoxication is associated with an increased risk of lactic acidosis, particularly in case of fasting or malnutrition or hepatic insufficiency.
Avoid consumption of alcohol and alcohol-containing medications.
lodinated contrast agents: Metformin must be discontinued prior to, or at the time of the image procedure and not restarted until at least 48 hours after, provided that renal function has been re-evaluated and found to be stable.
Combinations requiring precautions for use
Some medicinal products can adversely affect renal function which may increase the risk of lactic acidosis, e.g. NSAIDs, including selective cyclo-oxygenase (COX) II inhibitors, ACE inhibitors, angiotensin II receptor antagonists and diuretics, especially loop diuretics. When starting or using such products in combination with metformin, close monitoring of renal function is necessary.
Glucocorticoids (systemic and local routes), beta-2-agonists and diuretics have intrinsic hyperglycaemic activity. Inform the patient and perform more frequent blood glucose monitoring, especially at the beginning of treatment. If necessary, adjust the dosage of the antidiabetic drug during therapy with the other drug and upon its discontinuation. ACE-inhibitors may decrease the blood glucose levels. If necessary, adjust the dosage of the antidiabetic drug during therapy with the other drug and upon its discontinuation.
Metformin may decrease the anticoagulant effect of phenprocoumon. Therefore, a close monitoring is recommended.
Levothyroxine can reduce the hypoglycemic effect of metformin. Monitoring of blood glucose levels is recommended, especially when thyroid hormone therapy is initiated or stopped, and the dosage of metformin must be adjusted if necessary
Organic cation transporters (OCT): Metformin is a substrate of both transporters OCT1 and OCT2. Co-administration of metformin with
Inhibitors of OCT1 (such as verapamil) may reduce efficacy of metformin.
Inducers of OCT1 (such as rifampicin) may increase gastrointestinal absorption and efficacy of metformin.
Inhibitors of OCT2 (such as cimetidine, dolutegravir, ranolazine, trimethoprim, vandetanib, and isavuconazole) may decrease the renal elimination of metformin and thus lead to an increase in metformin plasma concentration.
Inhibitors of both OCT1 and OCT2 (such as crizotinib, olaparib) may alter efficacy and renal elimination of metformin.
Caution is therefore advised, especially in patients with renal impairment, when these drugs are coadministered with metformin, as metformin plasma concentration may increase. If needed, dose adjustment of metformin may be considered as OCT inhibitors/inducers may alter the efficacy of metformin.
USE IN SPECIFIC POPULATION
Pregnancy
Glimepiride
Pregnancy Category C
There are no adequate and well-controlled studies of Glimepiride in pregnant women. In animal studies there was no increase in congenital anomalies, but an increase in fetal deaths occurred in rats and rabbits at glimepiride doses 50 times (rats) and 0.1 times (rabbits) the maximum recommended human dose (based on body surface area). This foetotoxicity, observed only at doses inducing maternal hypoglycemia, is believed to be directly related to the pharmacologic (hypoglycemic) action of glimepiride and has been similarly noted with other sulfonylureas.
Glimepiride should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. Because data suggest that abnormal blood glucose during pregnancy is associated with a higher incidence of congenital abnormalities, diabetes treatment during pregnancy should maintain blood glucose as close to normal as possible.
Non-teratogenic Effects: Prolonged severe hypoglycemia (4 to 10 days) has been reported in neonates born to mothers receiving a sulfonylurea at the time of delivery.
Metformin
Teratogenic Effects: Pregnancy Category B.
Metformin was not teratogenic in rats and rabbits at doses up to 600 mg/kg/day, which represent 3 and 6 times the maximum recommended human daily dose of 2000 mg based on body surface area comparison for rats and rabbits, respectively. However, because animal reproduction studies are not always predictive of human response, Metformin HCI should not be used during pregnancy unless clearly needed. Labor and Delivery: The safety and effectiveness of Metformin used during labor and delivery has not been evaluated in human studies.
Fertility: Fertility of male or female rats was unaffected by metformin when administered at doses as high as 600mg/kg/day, which is approximately three times the maximum recommended human daily dose based on body surface area comparisons.
Lactation
Glimepiride
It is not known whether Glimepiride is excreted in human milk. During pre- and post-natal studies in rats, significant concentrations of glimepiride were present in breast milk and the serum of the pups. Offspring of rats exposed to high levels of glimepiride during pregnancy and lactation developed skeletal deformities consisting of shortening, thickening, and bending of the humerus during the postnatal period. These skeletal deformations were determined to be the result of nursing from mothers exposed to glimepiride. Based on these animal data and the potential for hypoglycemia in a nursing infant, a decision should be made whether to discontinue nursing or discontinue Glimepiride, taking into account the importance of Glimepiride to the mother.
Metformin
Studies in lactating rats show that metformin is excreted into milk and reaches levels comparable to those in plasma. Similar studies have not been conducted in nursing mothers. Thus, the potential for hypoglycemia in nursing infants after Metformin HCl oral solution may exist. Metformin is excreted into human breast milk. No adverse effects were observed in breastfed newborns/infants. However, as only limited data are available, breastfeeding is not recommended during metformin treatment. A decision on whether to discontinue breast-feeding should be made, taking into account the benefit of breast-feeding and the potential risk to adverse effect on the child.
Paediatric Use
Glimepiride The pharmacokinetics, efficacy and safety of glimepiride have been evaluated in pediatric patients with type 2 diabetes as described below. Glimepiride is not recommended in pediatric patients because of its adverse effects on body weight and hypoglycemia.
Safety and effectiveness Glimepiride/Metformin tablets in pediatric patients have not been established. Hence, it is contraindicated in children & adolescents below the age of 18 years.
Metformin
Safety and effectiveness in pediatric patients have not been established. Metformin is not recommended in pediatric patients below the age of 18 years.
Geriatric Use
Start with lowest dose in elderly patients due to higher risks of lactic acidosis, poor renal and hepatic functions.
Glimepiride
No overall differences in safety or effectiveness were observed between these patients and younger patients, but greater sensitivity of some older individuals cannot be ruled out.
Glimepiride is substantially excreted by the kidney. Elderly patients are more likely to have renal impairment. In addition, hypoglycemia may be difficult to recognize in the elderly. Use caution when initiating
Glimepiride and increasing the dose of Glimepiride in this patient population.
Metformin
Clinical studies of Metformin did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater
frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy and the higher risk of lactic acidosis.
Patients with renal or hepatic impairment
Glimepiride/Metformin tablet is not recommended in patients with renal or hepatic impairment.
Glimepiride
In case of severe renal or hepatic function disorders, a change over to insulin is required. In patients with low creatinine clearance, there was a tendency for glimepiride clearance to increase and for average serum concentrations to decrease, most probably resulting from a more rapid elimination because of lower protein binding.
To minimize the risk of hypoglycemia, the recommended starting dose of glimepiride is 1 mg daily for all patients with type-2 diabetes and renal impairment.
Metformin
A GFR should be assessed before initiation of treatment with metformin containing products and at least annually thereafter. In patients at an increased risk of further progression of renal impairment and in the elderly, renal function should be assessed more frequently, e.g. every 3-6 months.
UNDESIRABLE EFFECTS
Glimepiride and Metformin
The use of a combination of both compounds, either as a free combination or as a fixed combination, is associated with the same safety characteristics as the use of each compound separately.
The following CIOMS frequency rating is used, when applicable: Very common ≥10%; Common 1 and <10%; Uncommon ≥0.1 and <1%; Rare ≥0.01 and <0.1%; Very rare<0.01%, Unknown (cannot be estimated from available data).
Glimepiride
Metabolism and nutrition disorders: As a result of the blood-glucose-lowering action of glimepiride, hypoglycaemia may occur, which may also be prolonged. Possible symptoms of hypoglycaemia include headache, ravenous hunger, nausea, vomiting, lassitude, sleepiness, disordered sleep, restlessness, aggressiveness, impaired concentration, impaired alertness and reactions, depression, confusion, speech disorders, aphasia, visual disorders, tremor, pareses, sensory disturbances, dizziness, helplessness, loss of self-control, delirium, cerebral convulsions, somnolence and loss of consciousness up to and including coma, shallow respiration and bradycardia.
In addition, signs of adrenergic counter-regulation may be present such as sweating, clammy skin, anxiety, tachycardia, hypertension, palpitations, angina pectoris, and cardiac arrhythmias. The clinical picture of a severe hypoglycaemic attack may resemble that of a stroke.
The symptoms nearly always subside when hypoglycaemia is corrected.
Eye disorders: Especially at the start of treatment, there may be temporary visual impairment due to the change in blood glucose levels. The cause is a temporary alteration in the turgidity and hence the refractive index of the lens, this being dependent on the blood glucose level.
Gastrointestinal disorders: Occasionally, gastrointestinal symptoms such as nausea, vomiting, sensations of pressure or fulness in the epigastrium, abdominal pain and diarrhoea may occur. In isolated cases, there may be hepatitis, elevation of liver enzyme levels and/or cholestasis and jaundice, which may progress to life-threatening liver failure but can regress after withdrawal of glimepiride. Dysgeusia (frequency not known).
Blood and lymphatic system disorders: Changes in the blood picture may occur: Rarely, thrombocytopenia and, in isolated cases, leucopenia, haemolytic anaemia, erythrocytopenia, granulocytopenia, agranulocytosis or pancytopenia may develop. Cases of severe thrombocytopenia with platelet count less than 10,000/µl and thrombocytopenic purpura have been reported in post-marketing experience (frequency not known).
Skin and subcutaneous tissue disorders: Alopecia (frequency not known).
General disorders: Occasionally, allergic or pseudoallergic reactions may occur, e.g. in the form of itching, urticarial or rashes. Such mild reactions may develop into serious reactions with dyspnoea and a fall in blood pressure, sometimes progressing to shock. In the event of urticaria a physician must therefore be notified immediately. In isolated cases, a decrease in serum sodium concentration and allergic vasculitis or hypersensitivity of the skin to light may occur.
Investigations: Glimepiride, like all sulfonylureas, can cause weight gain (frequency not known).
Postmarketing Experience:
The following adverse reactions have been identified during post-approval use of glimepiride. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Serious hypersensitivity reactions, including anaphylaxis, angio-oedema, and Stevens-Johnson syndrome (SJS).
Haemolytic anaemia in patients with and without G6PD deficiency. Impairment of liver function (e.g. with cholestasis and jaundice), as well as hepatitis, which may progress to liver failure.
Porphyria cutanea tarda, photosensitivity reactions and allergic vasculitis.
Leucopenia, agranulocytosis, aplastic anaemia, and pancytopenia.
Thrombocytopenia (including severe cases with platelet count less than 10,000/µL) and thrombocytopenic purpura.
Hepatic porphyria reactions and disulfiram-like reactions.
Hyponatremia and syndrome of inappropriate antidiuretic hormone secretion (SIADH), most often in patients who are on other medications or who have medical conditions known to cause hyponatremia or increase release of antidiuretic hormone.
Metformin
Gastrointestinal symptoms such as nausea, vomiting, diarrhea, abdominal pain and loss of appetite (>10%) are very common: these occur most frequently during initiation of therapy and resolve spontaneously in most cases. To prevent these gastrointestinal symptoms, it is recommended that metformin be taken in 2 or 3 daily doses during or after meals. A slow increase of the dose may also improve gastrointestinal tolerability.
- Metallic taste (3%) is common.
- Mild erythema has been reported in some hypersensitive individuals. The incidence of such effects is regarded as very rare (<0.01%).
- A decrease of vitamin B12 absorption with decrease of serum levels has been observed inpatients treated long-term with metformin and appears generally to be without clinical significance (<0.01%).
However, cases of peripheral neuropathy in patients with vitamin B12 deficiency have been reported in post-marketing experience (frequency not known).
- Lactic acidosis (0.03 cases/1000 patient-years) is very rare.
- Hemolytic anemia (frequency unknown)
- Reduction of thyrotropin level in patients with hypothyroidism (frequency unknown)
- Hypomagnesemia in the context of diarrhea (frequency unknown)
- Encephalopathy (frequency unknown)
- Photosensitivity (frequency unknown)
- Hepatobiliary disorders: Reports of liver function tests abnormalities and hepatitis resolving upon metformin discontinuation.
In post marketing data and in controlled clinical studies, adverse event reporting in patients treated with Metformin SR was similar in nature and severity to that reported in patients treated with Metformin immediate release.
During treatment initiation, the most common adverse reactions are nausea, vomiting, diarrhoea, abdominal pain and loss of appetite, which resolve spontaneously in most cases.
Laboratory Tests:
Vitamin B12 concentrations: Metformin may lower serum vitamin B12 concentrations. Measurement of hematologic parameters on an annual basis is advised in patients on metformin and any apparent abnormalities should be appropriately investigated and managed.
OVERDOSE
Glimepiride
An overdosage of Glimepiride, as with other sulfonylureas, can produce severe hypoglycemia. Mild episodes of hypoglycemia can be treated with oral glucose. Severe hypoglycemic reactions constitute medical emergencies requiring immediate treatment. Severe hypoglycemia with coma, seizure, or neurological impairment can be treated with glucagon or intravenous glucose. Continued observation and additional carbohydrate intake may be necessary because hypoglycemia may recur after apparent clinical recovery.
Metformin
No cases of overdose were reported during Metformin clinical trials. It would be expected that adverse reactions of a more intense character including epigastric discomfort, nausea, and vomiting followed by diarrhea, drowsiness, weakness, dizziness, malaise and headache might be seen. Should those symptoms persist, lactic acidosis should be excluded.
Overdose of metformin hydrochloride has occurred, including ingestion of amounts greater than 50 grams. Hypoglycemia was reported in approximately 10% of cases, but no causal association with metformin hydrochloride has been established. Lactic acidosis has been reported in approximately 32% of metformin overdose cases. Metformin is dialyzable with a clearance of up to 170 mL/min under good hemodynamic conditions. Therefore, hemodialysis may be useful for removal of accumulated drug from patients in whom metformin overdosage is suspected.
PHARMACOLOGICAL PROPERTIES
Pharmacodynamic properties
Pharmacotherapeutic group: Blood glucose lowering drugs, Sulfonamides, urea derivatives and Biguanide oral hypoglycaemic agents.
Glimepiride
Glimepiride is an orally active hypoglycaemic substance belonging to the sulphonylurea group. Glimepiride primarily lowers blood glucose by stimulating the release of insulin from pancreatic beta cells. Sulfonylureas bind to the sulfonylurea receptor in the pancreatic beta-cell plasma membrane, leading to closure of the ATP-sensitive potassium channel, thereby stimulating the release of insulin.
Metformin
Metformin is a biguanide that improves glucose tolerance in patients with type 2 diabetes, lowering both basal and postprandial plasma glucose. Metformin decreases hepatic glucose production, decreases intestinal absorption of glucose, and improves insulin sensitivity by increasing peripheral glucose uptake and utilization. Metformin does not produce hypoglycemia in patients with type 2 diabetes or in healthy subjects except in special circumstances, and does not cause hyperinsulinemia. With metformin therapy, insulin secretion remains unchanged while fasting insulin levels and daylong plasma insulin response may actually decrease.
Pharmacokinetic properties
Absorption
The bioavailability of glimepiride after oral administration is complete. Food intake has no relevant influence on absorption, only the absorption rate is slightly diminished. Studies with single oral doses of glimepiride in healthy subjects and with multiple oral doses in patients with type 2 diabetes showed peak drug concentrations (Cmax) 2 to 3 hours post-dose.
Following a single oral dose of 1000 mg (2×500 mg tablets) metformin after a meal, the time to reach maximum plasma metformin concentration (Tmax) is achieved at approximately 7-8 hours. In both single and multiple-dose studies in healthy subjects, once daily 1000 mg (2×500 mg tablets) dosing provides equivalent systemic exposure, as measured by area-under-the-curve (AUC), and up to 35% higher Cmax, of metformin relative to the immediate release given as 500 mg twice daily.
Metformin sustained-release: The absolute bioavailability of a metformin 500 mg tablet given under fasting conditions is approximately 50-60%. Following a single oral dose of metformin sustained-release, Cmax is achieved within 4-8 hours. Peak plasma levels are approximately 20% lower compared to the same dose of metformin immediate release. Both high and low fat meals had the same effect on the pharmacokinetics of sustained release.
Distribution
Glimepiride has a very low distribution volume (approx. 8.8 litres), which is roughly equal to the albumin distribution space, high protein binding (>99%). After intravenous dosing in healthy subjects, the volume of distribution (Vd) was 8.8 L (113 mL/kg), and the total body clearance (CL) was 47.8 mL/min. Protein binding was greater than 99.5%.
The apparent volume of distribution (V/F) of metformin following single oral doses of 850 mg immediate release metformin hydrochloride averaged 654 ± 358 L. Metformin is negligibly bound to plasma proteins. Metformin partitions into erythrocytes, most likely as a function of time. At usual clinical doses and dosing schedules of metformin, steady state plasma concentrations of metformin are reached within 24-48 hours and are generally < 1 µg/mL. During controlled clinical trials, which served as the basis of approval for metformin, maximum metformin plasma levels did not exceed 5µg/mL, even at maximum doses.
Metabolism Glimepiride is completely metabolized by oxidative biotransformation after either an intravenous or oral dose. The major metabolites are the cyclohexyl hydroxy methyl derivative (M1) and the carboxyl derivative (M2). Cytochrome P450 2C9 is involved in the biotransformation of glimepiride to M1. M1 is further metabolized to M2 by one or several cytosolic enzymes. M2 is inactive. In animals, M1 possesses about one-third of the pharmacological activity of glimepiride, but it is unclear whether M1 results in clinically meaningful effects on blood glucose in humans.
Intravenous single-dose studies in healthy subjects demonstrate that metformin is excreted unchanged in the urine and does not undergo hepatic metabolism (no metabolites have been identified in humans), nor biliary excretion. Metabolism studies with extended-release metformin tablets have not been conducted.
Excretion
When “C-glimepiride was given orally to 3 healthy male subjects, approximately 60% of the total radioactivity was recovered in the urine in 7 days. M1 and M2 accounted for 80-90% of the radioactivity recovered in the urine. The ratio of M1 to M2 in the urine was approximately 3:2 in two subjects and 4:1 in one subject. Approximately 40% of the total radioactivity was recovered in feces. M1 and M2 accounted for about 70% (ratio of M1 to M2 was 1:3) of the radioactivity recovered in feces. No parent drug was recovered from urine or feces. After intravenous dosing in patients, no significant biliary excretion of glimepiride or its M1 metabolite was observed.
Renal clearance is approximately 3.5 times greater than creatinine clearance, which indicates that tubular secretion is the major route of metformin elimination. Following oral administration, approximately 90% of the absorbed drug is eliminated via the renal route within the first 24 hours, with a plasma elimination half-life of approximately 6.2 hours. In blood, the elimination half-life is approximately 17.6 hours, suggesting that the erythrocyte mass may be a compartment of distribution.
INCOMPATIBILITY
Not applicable.
SHELF LIFE
as per carton
STORAGE INSTRUCTIONS
Store protected from light & moisture, at a temperature not exceeding 30°C. Keep all medicines out of reach of children.
PACKAGING INFORMATION
As per carton
Manufactured by:
Pure & Cure Healthcare Pvt. Ltd.
(A subsidiary of Akums Drugs & Pharmaceuticals Ltd.)
Plot No. 26A, 27-30, Sector-8A, I.I.E., SIDCUL, Ranipur, Haridwar-249 403, Uttarakhand.
A WHO-GMP Certified Company
Marketed by:
TELIZAR HEALTHCARE LLP.
10, Prestige Trident, Lower Ground Floor, Airport Service Road, Domlur, Bangalore-560017, Karnataka, India
Registered Trademark – TM-Trademark under registration
Other Products
Tezapride M1
Teliglim-MV
Get in touch with us.
We’d love to hear from you.
Wish to know more about us?
We’re constantly working to develop innovative healthcare products
Providing real goodness to patients and making a difference to their lives is of prime importance for us at Telizar Healthcare.